
Melbourne University Law Review

|
|
Home
| Databases
| WorldLII
| Search
| Feedback
Melbourne University Law Review |
|
GENEVIEVE GRANT[*] AND DAVID M STUDDERT[†]
[In the civil justice system, medical expert witnesses act as brokers of what qualifies as legally recognised and compensable injury. Despite the central importance of their role, and continuing debate over the use of expert evidence, remarkably little empirical evidence is available about who medical experts are and what they do. This article reports findings from a study that built a detailed empirical profile of nearly 3000 instances of medical expert witness testimony, drawing from a sample of transport accident compensation cases in Victoria, Australia.]
CONTENTS
Injury is a leading cause of mortality, morbidity and permanent disability in Australia and globally.[1] More than 2.4 million Australians suffer from disabling long-term health conditions attributable to injuries.[2] The vast majority of these injuries occur at work (42 per cent), during exercise or sport (20 per cent), in transport accidents (17 per cent), or at home (12 per cent).[3]
Law’s most direct response to the problem of injury is through personal injury compensation, particularly for transport accident and work-related conditions. The compensation landscape in Australia is a complex combination of no-fault and statutorily modified common law arrangements.[4] Australia’s transport accident and workers’ compensation schemes handle caseloads and channel resources on a vast scale. They receive more than
180 000 new claims each year[5] and award billions of dollars in compensation. In 2009–10, the cost of workers’ compensation schemes alone, in
terms of benefits paid and operational and administrative costs, was
$7.3 billion.[6]
Many of the key determinations in adjudicating claims for com-
pensation — who is eligible, for how much, and for how long — turn on assessments of the claimant’s post-injury health state. Assessments of health states are largely, although not exclusively,[7] scientific and clinical constructions. Claimants, compensation agencies and adjudicators routinely turn to medical professionals to make these assessments. In this way, medical expert witnesses play a central role in the functioning of personal injury compensation systems.[8] Acting in their capacity as treating practitioners, or as hired medico-legal consultants, medical experts provide compensation systems with evidence relating to claimants’ injuries, treatment, impairment and disability.
The number of health professionals who devote their time to acting as medical experts is not large, especially in highly specialised fields like neurosurgery and orthopaedic surgery, where there are relatively small numbers of practitioners and the opportunity costs of time away from clinical practice are high. Some experts are regarded as better — more credible, authoritative, articulate, and persuasive — than others.[9] In other words, medical expertise is a finite resource and there is product differentiation. These are market conditions, and there is clear evidence that one flourishes in this area.[10] Expert evidence is the currency;[11] it is traded in support of the claims and counterclaims of injured parties and insurers. In this market, medical experts are the ‘injury brokers’[12] — agents of a crucial raw material in adjudicators’ determinations of what qualifies as legally recognisable and compensable injury.
Concerns about expert witnesses and the quality of their evidence abound in contemporary civil justice discourse. Costs and delays associated with expert evidence are common targets of criticism,[13] as are concerns about bias
and partisanship among experts.[14] A range of law reforms have been introduced in response to these concerns.[15] In Victoria, for example, the government recently moved to enhance judicial powers to regulate expert evidence in an attempt to curb the ‘wastage of court resources caused by the misuse and overuse of experts.’[16]
Unfortunately, these debates and reforms have unfolded in a data vacuum.[17] In particular, there has been very limited empirical investigation of the use of medical experts in Australian injury compensation claims.[18] How frequently and intensively are medical experts used? Which segments of the medical workforce step forward to play this role, and how representative are they of the specialty groups to which they belong? How is expert witness work distributed across the cadre of health professionals who take it on? Answers to such fundamental questions would add important information to policy discussions in this area, but are elusive. The lack of data is particularly troubling in the context of compensation schemes for workplace and transport injuries, where it is likely that the majority of medical expert witness activity occurs.
This article reports findings from a descriptive study of the characteristics of medical experts and their testimony in a large sample of personal injury cases. The cases were drawn systematically from decisions handed down in Victoria’s transport accident scheme over a seven-year period. Our goal was to build an empirical profile of these injury brokers, paying particular attention to statistical information with potential to shape and inform the ongoing
policy discussions about the proper role, use and oversight of expert
witnesses.
Medical expert witness practice creates many opportunities for empirical inquiry.[19] Previous studies have provided valuable, if only partial, perspectives on medical experts’ activities. This literature includes small-scale analyses of experts’ experiences of providing evidence;[20] investigations of the criteria lawyers use when selecting experts;[21] surveys of lawyers, judges and experts about their perceptions and experiences in court settings;[22] and reviews of insurer files to investigate the quality of reports[23] and levels of agreement between experts.[24] In addition, several studies in the United States have
described empirically the activity and characteristics of medical expert witnesses within particular jurisdictions,[25] specialties[26] and types of litigation.[27] However, there has been no such profiling of medical experts involved in civil litigation in Australia. Mapping the involvement of medical experts in injury compensation systems is an excellent place to start for reasons already mentioned — namely, the sheer scale of caseloads and costs in this setting, the crucial evidentiary role medical experts play, and the frequency with which the anecdotal evidence suggests they are employed.
Generic information appropriate for any basic descriptive profile of medical experts includes measures of their demographic characteristics (for example, age, gender and health profession or medical specialty), the intensity of their involvement (for example, mean number of experts per case), and the form their evidence takes (viva voce (live voice) or written). Examination of medical experts in the context of injury compensation systems introduces some additional measures of interest. For example, there is a fundamental difference between experts who provide evidence in their capacity as practitioners treating the claimant, and experts who assess or render views on the claimant’s condition in an independent, non-treating capacity.[28] Whereas a degree of randomness attends engagement of treating experts, non-treating experts are usually engaged at the discretion of parties to the claim. This makes them an especially interesting sub-group for analysis. Identifying ‘repeat players’ among non-treating experts, ascertaining their prominence in personal injury cases, and examining how they distribute their expertise between claimants and insurers has the potential to unlock information that is relevant to simmering policy questions about experts’ activities.
Most compensation claims are resolved without formal legal disputes,[29] much less disputes requiring adjudication in a court or tribunal. The majority of medical expert evidence associated with injury compensation systems is generated for and used in such non-litigated claims.[30] However, obtaining data on these claims is challenging. It generally requires securing access to the case files of insurers or compensation agencies, who are notoriously protective of this sensitive information. Claims that reach courts and tribunals are much more visible and accessible. For that reason, they have been the favoured source of data for profiling studies, and ours is no exception. Although these cases are a minority in numerical terms, and almost certainly not a representative cross-section of all claims, a focus on them for purposes of profiling medical experts is defensible, even desirable, for several reasons.
First, medical evidence adduced in adversarial hearings is often strongly contested. This is less likely to be the case in claims resolved outside formal legal forums, where the medical expert evidence may be concordant or involve differences that are small and amenable to negotiation.[31] Claims that proceed to courts and tribunals, by contrast, tend to involve fundamental disagreements over claimants’ eligibility for benefits, and those disagreements frequently hinge on which medical opinion the adjudicator accepts. In short, medical expertise tends to matter more in hearings.
Second, medical expert evidence also matters more in courts and hearings because it may assume precedential value there; how the decision-maker treats and interprets the evidence guides subsequent expert witness practice. For example, decided cases define the appropriate use of the standard metrics used in measuring physical impairment;[32] they also demonstrate the court or tribunal’s preparedness to acknowledge specific conditions or adopt certain articulations of the relationship between injury and loss.[33] Subsequently, these treatments of expert evidence in formal legal forums affect how such evidence is produced and used within that much larger body of cases resolved ‘in the shadow of the law’.[34]
Finally, medical expert evidence in hearings is particularly salient because most of the commentary and criticism, including that of judges, has targeted its role in these settings.[35] There is clearly an availability heuristic at work here.[36] Critics, especially judges, worry about uses of expert testimony in formal legal disputes because those are the uses they see. Nonetheless, this is a natural starting point for developing an evidence base on expert witnesses.[37] Visibility issues aside, concerns about cost and delay almost certainly loom larger in litigated cases.
For these reasons, together with the feasibility issues discussed, our study focused on a sample of cases involving medical expert witnesses that were adjudicated in courts and tribunals. None of the rationales offered for limiting the sample in this way forecloses the need to be cautious in generalising from study findings to the broader body of compensation claims.
The study used content analysis of court and tribunal decisions to profile a sample of medical expert witnesses who acted in transport accident compensation cases.[38] Content analysis has been the standard method used in the leading international empirical studies of expert witness practice published to date.[39] Its major components are the selection of cases for study, manual coding to record consistent information about each case, tests of the reliability of coding decisions, and data analysis.[40]
The study sample was drawn from cases adjudicated in courts and tribunals in relation to the transport accident compensation scheme operating in Victoria, Australia. The scheme, which was established by the Transport Accident Act 1986 (Vic) (‘TAA’), is hybrid in nature: it provides both no-fault benefits and restricted common law damages. The Transport Accident Commission (‘TAC’) administers the scheme. The TAC’s functions include the assessment and management of claims.[41]
No-fault benefits available to TAC claimants include medical and rehabilitation expenses and benefits designed to cover loss of earnings, loss of earning capacity, permanent impairment, death, and dependency.[42] Over and above these no-fault benefits, TAC claimants who have sustained a ‘serious injury’ due to the negligence of another may bring a common law claim for damages.[43] Claimants who are successful in common law actions may recover damages for pain and suffering, loss of enjoyment of life and economic losses associated with their injuries.[44]
Legal disputes may arise in relation to any of the benefits available to TAC claimants. Initial efforts to resolve these disputes typically begin with negotiation, informal administrative review and other processes specified by pre-action protocols,[45] reaching tribunals and courts for adjudication when resolution is not possible at those lower levels. Three formal legal forums hear first-instance disputes, applications and proceedings in relation to TAC benefits: the Victorian Civil and Administrative Tribunal (‘VCAT’), the County Court of Victoria, and the Supreme Court of Victoria. Administrative decisions of the TAC regarding acceptance of claims and claimants’ no-fault benefits are subject to review by VCAT. The County Court hears claimants’ applications for leave to proceed with common law actions,[46] and the County Court and Supreme Court hear damages claims.[47]
Data for the study was extracted from written decisions on TAC compensation claims issued by the three decision-making bodies described above. The sample frame consisted of unique decisions involving at least one medical expert witness that were handed down in the seven-year period from 1 July 2002 – 30 June 2009. For simplicity, we refer to the legal disputes that gave rise to these decisions as ‘cases’. The study timeframe was dictated by the decision publication practices of our largest source of data, the County Court of Victoria: its decisions could most reliably be identified and obtained from 2002 onward.[48] Before settling on this time period, we used data provided by
the TAC to confirm that a sufficiently large number of transport accident compensation decisions for meaningful analysis had been made in the study period.[49] This data also provided a check on the number of decisions ultimately acquired for the study. The study was confined to cases determined in the Melbourne registries of the relevant legal forums.[50]
Identifying cases from the County Court of Victoria that met our study eligibility criteria was somewhat challenging because not all of them are published. We began by reviewing the Court’s daily lists for the study period. Cases that were listed for judgment and involved the TAC or individuals as parties were flagged as candidate cases. All candidate cases were then cross-checked on CourtConnect, the Court’s online, publicly-accessible search facility for information about legal representation, filings, listings, and related activities in matters before the court. Where an electronic copy of the decision was available on the Court website, we downloaded it.[51] The rest of the decisions were obtained as hardcopy documents from Court files or by contacting associates of the relevant judges.[52]
Decisions of VCAT and the Supreme Court of Victoria were easier to identify because they are published routinely. We searched publicly accessible online databases for all cases in the period of interest that referred to the TAA.[53] Of 540 candidate cases containing references to the TAA, there was no online or written copy of the decision on the court’s file for 56 cases.[54] Hard copies of the rest of the decisions were obtained and reviewed closely to determine whether they met our sampling criteria. Eighty cases were excluded because there was no mention in the decision of the involvement of a medical expert witness.[55] Forty-four cases were excluded because they were appellate reviews of cases already included in the sample, or rehearings of earlier cases following a successful appeal.[56] These cases were effectively duplicates and to include them in the sample would have been double-counting because they did not introduce any additional experts or new expert evidence.[57] Finally, small numbers of cases were excluded because they involved non-TAC defendants[58] and concurrent workers’ compensation claims;[59] claims that did
not fall within the scope of the study’s focus on transport accident compensation cases; and decisions for which only incomplete written records could
be retrieved.
Melbourne transport accident decisions (2002/03 – 2008/09), identified through reviews of online databases, daily court and tribunal lists and court files (n = 540)
Study sample (n = 345)
(208 court and 137 tribunal decisions)
Ineligible decisions (n = 139)
• No medical expert (n = 80)
• Appeals and repeats (n = 44)
• Non-TAC defendant (n = 7)
• Concurrent workers’ compensation claim (n = 4)
• Incomplete record (n = 4)
Inaccessible decisions (n = 56)
Figure 1 provides an overview of the exclusions described above and shows how we derived the final study sample of 345 cases. There was a mean of 49 cases per year (range 31–67 cases). The sample is weighted toward the earlier years of the study timeframe because the number of cases reaching the determination stage has decreased since 2004–05, following the introduction of pre-action benefit and dispute resolution protocols in early 2005.[60]
Figure 1: Derivation of the Study Sample
Within the study sample of 345 cases, it was then necessary to identify a sample of medical experts for analysis. An expert medical witness was defined as a registrable health practitioner[61] whose provision of evidence in a case was referred to in the written court or tribunal decision. Experts provided evidence about the claimant’s condition, injury, treatment or prognosis for the purposes of the claim, based on their medical expertise.[62] Practitioners were not counted as experts for purposes of the study if they were mentioned in the decision in passing, without reference to an actual report; had provided their clinical notes, but no report; or had authored a report that was produced for purposes other than the transport accident claim at hand.[63] By excluding practitioners named in those capacities, the analysis retained a focus on experts whose engagement was substantive and related to the crux of the adjudicator’s decision.
Based on a review of previous international studies that have profiled expert witnesses, we generated a set of variables of interest. We then designed an instrument to facilitate collection of these variables from cases in the study sample. The instrument was developed and refined by two legally-trained coders (the first author and one other), who tested it on a selection of 15 cases drawn randomly from the study sample. We created a codebook to aid the
coding effort; it contained several coding rules aimed to standardise coding practice in areas of potential ambiguity and uncertainty.
The study variables are set out in Table 1 and a description of several key fields follows.
Table 1: Study Variables
|
Variable
|
Coding details
|
|
Case name
|
Case name
|
|
Case year
|
Financial year of decision
|
|
Forum
|
VCAT, County Court of Victoria, Supreme Court of Victoria
|
|
Adjudicator
|
Adjudicator name
|
|
Plaintiff solicitor firm
|
Firm name (if solicitor acting, otherwise self-representation noted)
|
|
Expert name
|
Expert name
|
|
Expert gender
|
Male, female or unknown
|
|
Expert specialty
|
Medical specialty (if medical practitioner) or health profession
|
|
Basis of expert involvement
|
Treating expert, non-treating expert or unknown
|
|
Party by whom non-treating expert was engaged
|
Plaintiff, defendant or unknown
(not applicable for treating experts)
|
|
Form of expert evidence
|
Viva voce or by written report only
|
Expert medical witnesses were medical practitioners, psychologists, physiotherapists, chiropractors, osteopaths, dental practitioners, podiatrists and optometrists.[64] Each identified expert was cross-checked by searching a national register of health practitioners maintained by the Australian Health Practitioner Regulation Agency (‘AHPRA’), which is online and publicly accessible.[65] The AHPRA register provides information on all registered practitioners’ gender, health profession and specialty (if any). We compared the information reported in the case on experts’ gender and qualifications with the same information in the register and relied on the register in the event of any discrepancy. For experts who did not appear on the AHPRA register, additional web searches were undertaken to obtain the characteristics of interest.[66]
This variable distinguished experts who were involved in their capacity as treating practitioners from experts who were involved in an independent, non-treating capacity.[67] For reasons noted above and elaborated in our findings below, this is an important distinction to make among experts in injury compensation claims.
This variable identified the party to the dispute who had engaged a non-treating expert. Decisions typically identified a particular non-treating expert as reporting to the plaintiff or defendant (or their solicitors), or grouped experts for a particular side together tagging them as, for example, ‘the plaintiff’s medico-legal witnesses’. Where an expert was described as having
been cross-examined by one party’s advocate, it was inferred that they had been engaged by the other party. We did not automatically code an expert whose evidence was relied on by a party as having been engaged by that party: in practice, a party could rely on the evidence of an expert who had been engaged by the other side.[68] Where it was unclear which party had engaged an expert, the expert’s engagement was coded as being unknown.
This variable indicated whether the expert attended court and gave viva voce evidence or provided evidence through a written report only. Viva voce presentations of evidence were routinely identifiable by explicit statements in the decision about the expert having given evidence in this manner, or mention of the expert having been ‘called’ or ‘cross-examined’.
The final instrument was applied to the decisions by the two coders. Working independently, each coder coded approximately half of the sample, entering values for variables of interest into an electronic workbook. The workbook was pre-filled with the administrative details for each case, which had been obtained directly from court and tribunal registries, decisions and online databases.[69] For each case, the coder checked the administrative details recorded in the workbook against values for those variables in the text of
the decision.
To test the degree of agreement between coders, a random selection of
10 per cent of cases (n = 34) was re-reviewed by a second coder who was blinded to the occurrence and results of the first review. The testing demonstrated 96 per cent agreement between coders in enumerating an identical list of experts for each case. There was also excellent agreement between coders on variables that required implicit judgments. Measures of inter-rater reliability (kappa scores) for four of the key variables are shown in Table 2.[70]
Table 2: Results of Reliability Testing
|
Variable
|
Percentage
agreement
|
к score (95%
confidence interval)
|
|
Expert gender
|
93.8%
|
0.80 (0.72–0.88)
|
|
Form of expert evidence
|
93.5%
|
0.81 (0.71–0.90)
|
|
Party by whom expert was engaged
|
86.4%
|
0.82 (0.77–0.87)
|
|
Basis of expert involvement
|
91.9%
|
0.84 (0.79–0.89)
|
Most of the general analyses involved calculation of simple counts and percentages. To test for significant differences between variables of interest, we used chi-square and t-tests as appropriate, and interpreted p-values less than 0.05 as indicative of statistically significant differences.
The sample consisted of 345 cases in which a decision was handed down between 1 July 2002 and 30 June 2009. There were 137 VCAT decisions, 207 County Court of Victoria decisions and one Supreme Court of Victoria decision.[71]
A depiction of medical expert witnesses and their testimony calls for several different levels of analysis. The level of analysis best suited to describing characteristics differs across variables. For example, the number of treating and non-treating experts engaged to provide evidence is best examined at the case level. Analyses at the expert level are the most informative way to explore the concentration of expert witness activity. And it is appropriate to analyse the demographic characteristics of experts — for example their gender or medical specialty composition — at what we call the ‘involvement level’. An involvement refers to each separate instance in which an expert is engaged. Any given case may have multiple involvements, corresponding to multiple unique experts.[72] The presentation of findings that follows moves between these levels of analysis, as appropriate for the characteristics under analysis.
The cases involved an average of nine medical expert witnesses per case (range 1–27), approximately half of whom were non-treating experts (mean of five, range 0–21). In a third of cases, seven or more non-treating experts
were engaged.
Fifty-nine different adjudicators (judges and tribunal members) decided the cases, and many decided multiple cases (overall mean of six cases
per adjudicator, range 1–34). The 10 adjudicators with the largest numbers
of cases accounted for 187 of them, or 54 per cent of all cases in the
study sample.
Sixty-three firms of plaintiff solicitors acted in at least one case (mean of six cases per firm, range 1–58) and claimants were self-represented in 14 cases. The 10 firms of plaintiff solicitors that acted in the most cases accounted
for 203 cases, or 59 per cent of all cases. The TAC was the respondent or defendant in all cases and was always represented by its in-house solicitors.
Among the 345 cases, there was a total of 2984 medical expert witness involvements (hereafter, ‘involvements’). Sixty per cent of these involvements were by non-treating experts (1794 of 2984) (Table 3). Four in every five involvements consisted of expert evidence presented by written report, rather than viva voce, and this proportion did not differ between treating and non-treating experts.
Table 3: Incidence and Form of Expert Medical Evidence
|
Basis of expert engagement
|
|
Expert
involvements (n)
|
Form of evidence
|
|||
|
Report n (%)
|
Viva voce n (%)
|
|||||
|
Treating
|
|
1113
|
887
|
(79.7%)
|
226
|
(20.3%)
|
|
Non-treating
|
|
1794
|
1439
|
(80.2%)
|
355
|
(19.8%)
|
|
Unknown
|
|
77
|
77
|
(100.0%)
|
0
|
(0.0%)
|
|
Total
|
|
2984
|
2403
|
(80.5%)
|
581
|
(19.5%)
|
Figure 2 shows a breakdown of the involvements of non-treating medical experts by their clinical specialties. Doctors dominated, accounting for 94 per cent (1693 of 1794) of all involvements. Orthopaedic surgeons (28 per cent of involvements) and psychiatrists (25 per cent) were the most frequently engaged; these two types of specialists accounted for 53 per cent of all involvements.[73] Overall, 46 per cent (829 of 1794) of all non-treating expert involvements were by surgeons.[74]
Among the 4 per cent of involvements by clinicians other than doctors, neuropsychologists and psychologists were the most common, accounting for 3 per cent and 1 per cent of involvements, respectively. For 2 per cent (n = 28) of non-treating expert involvements, it was not possible to determine the expert’s specialty or health profession.
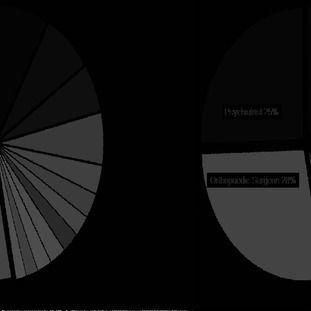
Figure 2: Non-Treating Expert Involvement by Specialty
The high prevalence of involvements by non-treating orthopaedic surgeons and psychiatrists shown in Figure 2 was also evident in analyses at the case level. Seventy per cent of cases (242 of 345) involved at least one non-treating orthopaedic surgeon, and almost two thirds of these cases (155 of 242) involved multiple orthopaedic surgeons. The involvement of non-treating psychiatrists in cases showed similar patterns: they were prevalent (at least one was engaged in 61 per cent of all cases) and involvements tended to group within cases (three quarters of cases with at least one psychiatrist had two or more).
Non-treating experts were involved in an average of 4.7 cases (range 1–67), but this average masks a dramatic skew in the distribution of those cases among experts. The key feature of that skew is the heavy concentration of expert witness activity within a small group of ‘repeat players’.
The first column of figures in Table 4 shows the number of non-treating experts in various ‘bands’ of case numbers. These bands indicate the total number of cases in which the non-treating experts were involved over the study period. Half (194 of 382) of all non-treating experts were involved in only one case and 12 per cent (46 of 382) were involved in more than 10 cases.
The second column of figures in Table 4 indicates the number and proportion of all involvements accounted for by experts in each band. Although only 4 per cent of non-treating experts were involved in 23 or more cases, the frequency of their involvements meant that this group accounted for 30 per cent of all involvements. The 30 experts who were involved in 16 or more cases accounted for nearly half of all involvements. The shaded section of the table highlights this remarkable concentration.
Table 4: Distribution of Non-Treating Experts across Cases
|
Case total in study period
|
Non-treating
experts
n %
|
Involvements by
non-treating experts
n %
|
||
|
1
|
194
|
51%
|
194
|
11%
|
|
2 to 3
|
79
|
21%
|
186
|
10%
|
|
4 to 6
|
40
|
10%
|
191
|
11%
|
|
7 to 10
|
23
|
6%
|
181
|
10%
|
|
11 to 15
|
16
|
4%
|
216
|
12%
|
|
16 to 22
|
15
|
4%
|
294
|
16%
|
|
23 or more
|
15
|
4%
|
532
|
30%
|
|
Total
|
382
|
100%
|
1794
|
100%
|
The small coterie of non-treating experts who appear frequently are likely to be particularly influential witnesses in the litigation under study, not least because of the large proportion of all decisions that consider their opinions. We therefore conducted a series of additional sub-analyses to describe some basic characteristics of this frequent expert (‘FE’) group. We defined a FE as a non-treating expert who had provided evidence in seven or more study cases.[75] Seven cases was selected as the threshold for FE status as it required that FEs averaged at least one case per year across the seven-year study period. The approximate age of each FE was calculated by adding 24 years to the number of years since the FE’s first professional registration as recorded on the AHPRA register.[76]
There were 69 FEs in total. They provided evidence in 317 cases and amassed 1223 involvements over the study period. In proportional terms, these counts correspond to 18 per cent of non-treating experts, 92 per cent of cases and 68 per cent of non-treating involvements. On average, FEs were involved in 18 cases, or 2.8 cases per year.[77] All but two of the FEs were doctors, chiefly surgeons (n = 29), psychiatrists (n = 18) and neurologists
(n = 6).[78] FEs were predominantly older men. Only six (9 per cent) of them were women, significantly lower (p < 0.01) than the proportion of female specialists in the medical workforce.[79] At an average age of 61 years, FEs were also significantly older (p < 0.001) than the average age of medical specialists
(50 years).[80] The distinctive specialty profile of FEs does not explain this age difference. For example, the mean age of surgeon FEs was 66 years, significantly older (p < 0.001) than the average age of surgeons nationwide
(52 years).[81]
The fact that FEs, by definition, had been involved in multiple cases created an opportunity to explore the issue of alignment. Using information on which side of the litigation FEs had provided evidence for, we calculated the ‘split’ between plaintiff and defendant work for each FE. Figure 3 presents the results. Each horizontal bar in the figure (even as it crosses the central column) represents a single FE. The left-hand portion of the bar represents cases in which the FE was engaged by the TAC and the right-hand portion represents cases in which the FE was engaged by the claimant. The number shown in the column between the two portions of each bar reports the number of cases in which it was not possible to determine which party engaged the expert.
This breakdown of FE activity conveys several findings. Nearly half (48 per cent) of the FEs were engaged exclusively by one side, and most FEs were engaged far more frequently by one side than the other. Among cases in which the engaging party was identifiable, 8 in 10 FEs gave evidence for the same side in at least three quarters of their cases. In short, there is clear evidence that FEs tended to consistently assume the role of either plaintiff or defendant experts.
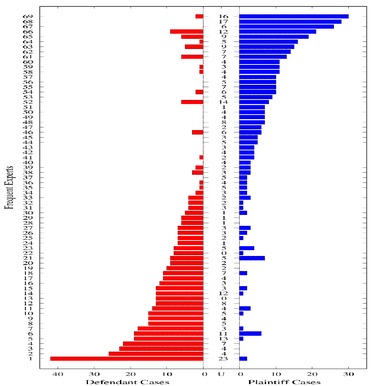
Figure 3: Alignment of Frequent Experts
The utter dominance of males among FEs was arguably the most striking finding in the foregoing sub-analysis of non-treating experts. While this finding is of interest in the FE sub-sample, the extent to which it is true for the study sample as a whole is also of interest.
Analysis of the gender composition of all medical expert witness involvements in the study sample showed that female experts accounted for 10 per cent of involvements. Table 5 shows this result. It also shows a breakdown of gender by reference to whether the expert involvements were in a treating or non-treating capacity. Female experts had significantly lower (p < 0.001) representation among non-treating experts (7 per cent) than they did among treating experts (14 per cent). In other words, although female representation among experts was low across the board, it was especially low for involvements where the parties to the litigation had direct control over the choice
of witnesses.
Table 5: Basis of Expert Involvement by Gender[82]
|
Expert gender
|
Basis of expert involvement
|
Total
|
||||||
|
Treater
|
Non-treater
|
Unknown
|
||||||
|
Female
|
147
|
14%
|
126
|
7%
|
12
|
19%
|
285
|
10%
|
|
Male
|
922
|
86%
|
1662
|
93%
|
52
|
81%
|
2636
|
90%
|
|
Total
|
1069
|
100%
|
1788
|
100%
|
64
|
100%
|
2921
|
100%
|
A second way in which female experts were under-represented was their low visibility in legal forums. Female non-treating experts provided viva voce evidence on only 19 occasions, whereas male non-treating experts did so on 334 occasions.[83]
One logical objection to the finding of female under-representation in the study sample relates to specialty. We have already shown that doctors from particular specialties and sub-specialities, most notably surgical ones, dominate the expert witness population. That there is a low number of female surgeons is a well-documented workforce statistic.[84] Are we, then, merely observing a specialty effect in different guises? A specialty-specific analysis of female expert involvements that compares their representation in the national workforce addresses that question.
Table 6: Leading Specialties of Non-Treating Medical Experts, by Gender
|
Medical specialty
|
Expert involvement in
study cases
|
Proportion female in Australian specialty
workforce (%)[85]
|
||
|
Total (n)
|
Female
|
n (%)
|
||
|
All medical specialties
|
1681
|
84
|
5%
|
22%
|
|
Orthopaedic surgery
|
494
|
0
|
0%
|
3%
|
|
Psychiatry
|
454
|
39
|
9%
|
31%
|
|
Neurology
|
149
|
20
|
13%
|
14%
|
|
Neurosurgery
|
104
|
0
|
0%
|
9%
|
|
All surgery
|
829
|
0
|
0%
|
8%
|
Table 6 shows the results of a simple comparison along these lines. A gross gender disparity remains evident, both for specialist medical experts as a whole and for four of the most prevalent specialties. The only specialty that approached comparability was neurology (13 per cent of involvements and 14 per cent of the medical workforce). It should be noted, however, that 18 out of the 20 non-treating expert involvements by a female neurologist were provided by a single practitioner. Similarly, two female FEs accounted for 34 of the 39 non-treating psychiatric opinions provided by female psychiatrists.
By shedding light on the general characteristics of medical expert evidence and the health professionals who provide it in a large injury compensation system, this study creates a body of information that has been missing from contemporary Australian policy debates in this area. This section considers
the implications of four strands in our findings: the intensity of expert involvement; the form in which evidence is typically given; the prominence of frequently used experts; and the near absence of female experts.
Our findings demonstrate clearly that litigation occurring in and around Victoria’s transport accident scheme relies heavily on medical expert evidence. Of the 484 cases in our sample frame for which it was possible to obtain a decision, 404 (84 per cent) involved one or more medical experts.[86] This highlights the frequency with which experts are used and hints strongly at their influence in legal disputes in this jurisdiction. Within cases, we also found intensive use of medical experts, with an average of nine engaged per case, more than half of whom were non-treating experts.
A previous study of 361 compensation-related appeals in the federal
Administrative Appeals Tribunal also found a high proportion of cases involved experts (84 per cent), but far fewer experts per case than we observed.[87] This suggests that intensity of use of medical experts within cases may differ widely across jurisdictions.[88] The more intensive use of medical
experts is likely due to a combination of structural and procedural differences between jurisdictions (for example, evidentiary requirements) and differences in legal cultures and practices. Disentangling the drivers of varying levels of usage of medical experts would require comparative studies.
Within the large numbers of medical expert witnesses involved in cases, we observed specialty clusters. Analyses of the two most prevalent specialty groups bore this out. In about 40 per cent of cases in which a non-treating psychiatrist was involved, at least three non-treating psychiatrists were involved; in a quarter of cases in which a non-treating orthopaedic surgeon was involved, at least three were involved. One possible explanation for such clustering is that, in an adversarial system, the decision of one party to engage an expert can trigger a kind of arms race. For example, one side’s engagement of an orthopaedic surgeon presses the other side to do the same, or risk being outgunned on an evidentiary point. Indeed, responding with two authoritative opinions from orthopaedic surgeons may trounce the opponent’s line of argument, but the opponent will have incentives to match that move. And so goes the arms race.
The involvement of large numbers of expert witnesses probably has negative implications for the efficiency of litigation. The cost of expert evidence can be a very substantial component of litigation budgets. With an average of nine experts per case, this is certain to be true for many of the cases analysed in our study. Expert evidence is also a notorious source of delay in claim processing.[89] The process of recruiting experts, coordinating their involvement, awaiting their written evidence, and then incorporating that evidence into legal documents and argumentation extends case timelines. In addition, non-treating experts usually examine the claimant in person, sometimes several times, and there is emerging evidence that an accumulation of such non-therapeutic engagements may slow a claimant’s recovery.[90]
Despite the inverse relationship between numbers of experts engaged and efficiency, it would be wrong to jump to the conclusion that engagement of
large numbers of medical experts is always undesirable. Our study quantified
the number of experts and expert involvements; it did not assess the appropriateness of their involvement or the quality of their evidence. In other words, our analysis, and the discussion so far, has not considered the benefits side of the equation. When medical experts are retained and used appropriately, they should add value. So the example of the arms race in orthopaedic surgeon experts described above is not necessarily a counterproductive phenomenon. If the dispute turns on a difficult clinical question in orthopaedics on which there is likely to be a range of expert views, having several experts from the same specialty may help the adjudicator in getting to the ‘right’ decision — it is the forensic equivalent of a patient seeking second and third opinions to inform an important decision about treatment. In addition, many of the plaintiffs in the study cases had complex health problems and had been treated over many years leading up to the litigation.[91] Both of these factors are potential multipliers on the cast of medical experts needed to provide a full account of health-related evidentiary matters.
Nonetheless, although our study does not address the quality or necessity of medical expert evidence, its findings about the very high frequency and intensity with which medical experts are used in transport accident cases in Victoria underscore concerns about the potential for inappropriate and excessive use of experts. At the very least, the volume we detected points to a pressing need for future research to tackle the quality question.
Medical experts provided viva voce evidence in only 1 in 5 involvements; the rest of the time their evidence was adduced solely in written form. This heavy weighting toward written reports, even among cases that reach formal legal hearings, bucks the conventional wisdom about the role of expert witnesses. Its policy implications are unclear. On the one hand, it is almost certainly a cheaper vehicle for obtaining expert opinion. On the other hand, resolving differences of medical opinion on the basis of written reports in the absence of
oral evidence creates challenges for decision-makers.[92] It limits opportunity for the decision-maker to probe key statements or witness credibility and forecloses opportunities for experts to challenge each other.[93]
A cadre of fewer than 50 experts provided nearly 60 per cent of the non-treating medical evidence examined in our study. Nearly all were clearly identifiable as plaintiff or defendant experts, based on the pattern of their involvements. Particular plaintiff firms and adjudicators were also involved in a disproportionately large share of the cases.[94] Taken together, these findings sketch a picture of an entrenched community of repeat players, who know each other and handle most of the cases.[95]
Edmond cautions that reference to ‘repeat player’ status in expert evidence discourse can have a stigmatising effect. ‘Defence experts’, he argues, are often exempted from the terminology, and the stigmatisation of experts specialising in litigation ‘operates to the detriment of plaintiffs’ by reducing access to experts and therefore access to justice.[96] Our findings suggest it is impossible to present an accurate portrait of expert witness activity without recognising and considering the role of repeat players. The influence of this remarkably small group of doctors penetrates a majority of cases. Policies and reforms that ignore their existence may miss the mark. That said, it is important to recognise that repeat players appear to exist on both sides of the litigation. In the pool of transport accident cases that formed our sample, there were
similar numbers of repeat players engaged for defendants and plaintiffs, respectively; both sets of frequent witnesses were involved in large proportions of the total pool of cases; and both showed the consistency of alignment with one side.
The deeper question is one of effect, not terminology. What implications does, or should, the central role of an aligned group of frequent non-treating experts have for optimal design of rules and policies that govern medical expert evidence?
It would be remiss not to recognise that frequent experts are likely to improve accessibility to medical expertise and bring valuable stability to the systems in which they work. Injury compensation systems, like the one we focused on, rely on medical experts to progress vast caseloads, and to fulfil their compensation and dispute resolution functions. It should also be remembered that although expert work can be well-remunerated, the remuneration for many specialists would compare unfavourably with earnings from clinical work. This is especially likely to be the case for surgeons, who played such a prominent role in medical expert work in our sample.
In this environment, schemes and litigants may have sound reasons to opt for experts who are experienced in conducting the work and willing to take on more. Of all potential expert witnesses, those who are tried and tested may be best placed help the civil justice system achieve its objectives of timeliness, accessibility, consistency and predictability in outcomes.[97] There is tension between this realpolitik of expert witness selection and the discomfort created by the notion of the ‘professional expert’.[98]
Nonetheless, the bases of that discomfort cannot be ignored. For many, the portrait of the ‘professional witness’ that our findings sketch may deepen concerns about conflicts of interest, independence and quality of expertise. Again, it seems impossible to assess the legitimacy of those concerns, or to gauge the extent to which they undo the advantages of frequent experts outlined above, without reference to the quality of evidence frequent experts provide. Measures of the quality of evidence provided by frequent witnesses are a crucial arbiter in determining whether this type of expertise is
problematic.
Unfortunately, that measurement exercise is not straightforward. Indirect indicia — such the extent of expert alignment — are insufficient proxies for low quality evidence.[99] As Edmond has argued, while it is reasonable to be attentive to the effects of various forms of bias,[100] in isolation, attributions of bias, alignment and vested interests do not provide concrete tools for measuring expertise and expert performance.[101] We are optimistic, however, that measurement in this area may be possible. Other fields, such as health services research, have successfully developed ‘appropriateness’ criteria for assessing quality, and then enlisted neutral third-party experts to apply these criteria.[102] We see no reason why a field of legal services research could not rise to do the same for aspects of litigation such as expert witness evidence.[103] The fact that the methods for generating these measures in legal settings are un- or underdeveloped does not mean it is infeasible.
Even without the benefit of reliable measures of the quality of expert evidence, signs that the market for medical expertise is a closed shop, reserved for doctors of a particular demographic profile, might be regarded as inherently problematic. We found some evidence of this: our results showed a mismatch between the age and gender profile of medical experts and that of the professional communities to which they belong.
In particular, there was a disproportionately large presence of older males among non-treating experts. Recognising that nearly half of all non-treating
experts were surgeons, we tested whether this result was the artefact of specialties whose ranks are dominated by older males. It was not. Even within specialties, female experts were grossly under-represented relative to their numbers in the medical workforce.
This profiling suggests that medical expert work is an endeavour male doctors turn to late in their careers. For surgeons, whose average age in the FE group was 66 years, this is probably a career path that opens up for many as their operating skills begin to decline and the rigours of a busy clinical life become too taxing.[104] But part of the explanation for the prominence of these demographic characteristics is likely to lie in demand-side factors as well. For litigants, the extensive clinical experience of older doctors is likely to be attractive. Male doctors at the end of their clinical careers may be perceived by those who engage them as exuding authority and having the capacity to persuade decision-makers in a way that experts who are younger and female cannot.[105] (It cannot hurt that many of the decision-makers in courts and tribunals are males of a similar vintage.)
Supply-side and demand-side factors come together in the economics of expert witness markets. The fees mid-career subspecialists in private practice would need to charge for expert witness work, in order to offset their time away from clinical practice, are likely to be prohibitively expensive for many litigants. As the hours spent in clinical practice decrease in late career, however, so do the opportunity costs associated with taking on medico-
legal work.
On closer analysis, then, some of these selection effects look benign, perhaps even socially desirable. However, the near total absence of women among injury brokers remains troubling. Even among psychiatric expert witnesses in our study — a specialty with a comparatively high proportion of female practitioners — few were female. The absence of female injury brokers raises questions that have parallels in the representation of women in other visible roles in courtroom settings — namely judges and barristers. The
numerical equality of women law graduates with their male counterparts has not translated into equality in the senior ranks of the legal profession, the Bar or Bench.[106] This empirical reality flies in the face of the still common suggestion that increased equality in the representation of women in these areas is a ‘matter of time’.[107]
Construing the absence of women among medical experts as ‘just’ an equity issue, however, casts the problem too narrowly. Previous research has documented gender differences in the way doctors approach clinical practice.[108] For example, there is evidence that female practitioners ‘engage in communication that more broadly relates to the larger life context of patients’ conditions by addressing psychosocial issues’,[109] reflecting a more patient-centred style of communication.[110] It is reasonable to expect that these gender differences could extend into the forensic context, though this remains to be determined.[111]
The health state assessments that medical experts are called upon to make, as we noted above, are partly clinical and scientific in nature, but they are also heavily contextualised social constructions. For example, the ability of some TAC claimants to access common law benefits turns on a qualitative determination of what qualifies as ‘serious’ injury.[112] Non-clinical life impacts are a legitimate component of this determination. Research on quality of life has demonstrated that women weigh such impacts differently to men.[113] Thus, to the extent the opinions of medical experts extend beyond strictly clinical
evaluations, there is an even stronger basis for worrying that the absence of women among experts leads to the production of qualitatively different evidence than would come from a more gender-balanced expert pool; indirectly, then, it may also lead to different case outcomes.
More generally, the invisibility of female experts threatens the integrity and legitimacy of compensation systems. The historical inequity experienced by women in legal processes manifested in the exclusion of women from access to roles in courts, on the basis of ‘the myth that women were naturally frail, could not hold up under the rigors of court work, and would thus interfere with the efficient functioning of the court system.’[114] The lack of female experts in the cases and legal forums in the jurisdiction we studied has the expressive function of communicating that female health professionals do not have sufficient expertise to join the ranks of injury brokers in compensation systems. In this way, the operation of the market for injury brokers constitutes a social practice that is both reflective and constitutive of the legal culture in compensation systems.[115]
In summary, medical expert witnesses in the compensation system we studied are extremely unrepresentative — in terms of age and gender — of the professional groups from which they come. In some respects, that lack of representativeness may be inconsequential, but it is difficult to draw that conclusion about the absence of women. Their exclusion from the market for experts is a market failure, and the negative externalities arising from it demand further attention.[116]
This study is the largest of its kind to be conducted in Australia to date. It offers several novel and useful insights into the make-up and practices of medical expert witnesses employed in an injury compensation system. Two methodological strengths warrant mention because they are not standard features of the international empirical research on expert witnesses. First, the
sample of cases used to identify and characterise medical expert witnesses was drawn systematically from decisions handed down by all relevant judicial bodies over an extended period. This approach allowed us to generalise with confidence from our findings to the wider pool of transport accident cases in Victoria. Second, our ability to compare certain characteristics of the witnesses to corresponding national data permitted some firm conclusions about representativeness.
The study also has several weaknesses that need mentioning. First, although our sampling methodology provided a strong basis for generalising findings to the compensation scheme that covers transport accidents in Victoria, the generalisability to other compensation systems and other states may be limited. Second, the study relied on the reports of expert witness involvement contained in the written decisions of judges and tribunal members. It is likely that not every expert involvement is mentioned in every case and so some experts may have been missed.[117] Finally, the decision to restrict the study sample to cases that reached courts and tribunals means the analysis relates to the peak of the ‘dispute pyramid’. Although there are compelling reasons to focus on expert witness activity there,[118] a much larger body of claims are settled outside formal legal forums, and the roles and types of medical experts in those claims may be different.
This study provides a detailed empirical profile of expert witnesses and their evidence in litigated cases within a large injury compensation system. Its key findings include the high frequency and intensity with which medical experts are used, the pervasive role of experts who appear frequently in a non-treating capacity, and the idiosyncratic profile of these experts, most notably their gender imbalance. The article considered the normative implications of these and other findings.
There is much new information here to inform future debates about the proper uses and roles of medical expert witnesses in injury compensation systems. However, empirical legal research tends to sharpen normative questions, not resolve them. A crucial missing piece of empirical information in the policy discussions and academic commentary around medical expert witnesses is whether and to what extent the quality of evidence differs across the groups of experts identified in this study. Addressing that question will probably require the development of new methods of empirical legal research, particularly appropriate measures of quality. It is worth trying. That information, coupled with the kind of descriptive evidence our study provides, could constitute an empirical evidence base powerful enough to reshape the rules and policies that determine how medical expertise is deployed in medico-legal forums.
[*] BA, LLB (Hons), PhD (Melb); Research Fellow, Melbourne School of Population and Global Health, The University of Melbourne.
[†] BA, LLB (Melb), ScD, MPH (Harv); Professor and ARC Laureate Fellow, Melbourne Law School and Melbourne School of Population and Global Health, The University of
Melbourne.
[1] Rafael Lozano et al, ‘Global and Regional Mortality from 235 Causes of Death for 20 Age Groups in 1990 and 2010: A Systematic Analysis for the Global Burden of Disease Study 2010’ (2012) 380 Lancet 2095, 2110, 2113, 2119; Christopher J L Murray et al, ‘Disability-Adjusted Life Years (DALYs) for 291 Diseases and Injuries in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010’ (2012) 380 Lancet 2197, 2203, 2218; Stephen J Begg et al, ‘Burden of Disease and Injury in Australia in the New Millennium: Measuring Health Loss from Diseases, Injuries and Risk Factors’ (2008) 188 Medical Journal of Australia 36, 37–9; Raymond A Cripps and James E Harrison, ‘Injury as a Chronic Health Issue in Australia’ (NISU Briefing No 13, Australian Institute of Health and Welfare National Injury Surveillance Unit, 15 September 2008) 3 <http://www.aihw.gov.au/ publication-detail/?id=6442468148> .
[2] Australian Bureau of Statistics, 2009–10 Year Book Australia (ABS Catalogue No 1301.0, 2010) 356. See also Australian Bureau of Statistics, 2007–08 National Health Survey: Summary of Results (ABS Catalogue No 4364.0, August 2009) 12.
[3] Australian Bureau of Statistics, 2009–10 Year Book Australia, above n 2.
[4] For example, each of the nine major workers’ compensation schemes operating in Australia (the state and territory schemes and the Commonwealth Comcare scheme) provide no-fault compensation for occupational injury and disease; only the Northern Territory and South Australian schemes do not allow common law claims. For an overview of these arrangements, see Safe Work Australia, Comparison of Workers’ Compensation Arrangements in Australia and New Zealand (2012). Varying levels of no-fault compensation for transport accident injury are provided in Victoria, New South Wales, Tasmania and the Northern Territory: see Transport Accident Act 1986 (Vic) (‘TAA’); Motor Accidents Compensation Act 1999 (NSW); Motor Accidents (Lifetime Care and Support) Act 2006 (NSW); Motor Accidents (Liabilities and Compensation) Act 1973 (Tas); Motor Accidents (Compensation) Act 1979 (NT). Queensland, Western Australia, South Australia and the Australian Capital Territory do not provide any no-fault compensation for transport accident injury, and common law claims are excluded in the Northern Territory: Motor Accidents (Compensation) Act 1979 (NT) s 5(1).
[5] Genevieve Grant and David M Studdert, ‘Poisoned Chalice? A Critical Analysis of the Evidence Linking Personal Injury Compensation Processes with Adverse Health Outcomes’ [2009] MelbULawRw 29; (2009) 33 Melbourne University Law Review 865, 867 n 9.
[6] Safe Work Australia, Key Workers’ Compensation Information, Australia (2012) 5 <http://www .safeworkaustralia.gov.au/sites/swa/about/publications/pages/key-wc-information-2012> .
[7] Some tests of eligibility rely on qualitative assessments of the impact of an injury on a claimant’s life: see, eg, TAA s 93(17); Accident Compensation Act 1985 (Vic) s 134AB(38). Additionally, legal scholars have highlighted the role of social and political considerations in shaping the assessment of injury in compensation settings: see, eg, Ellen Smith Pryor, ‘Flawed Promises: A Critical Evaluation of the American Medical Association’s Guides to the Evaluation of Permanent Impairment’ (1990) 103 Harvard Law Review 964; David M Engel, ‘Lumping as Default in Tort Cases: The Cultural Interpretation of Injury and Causation’ (2010) 44 Loyola of Los Angeles Law Review 33, 37–8, 46; Marc Galanter, ‘The Dialectic of Injury and Remedy’ (2010) 44 Loyola of Los Angeles Law Review 1; Reg Graycar, ‘Damaging Stereotypes: The Return of “Hoovering as a Hobby”’ in Janice Richardson and Erika Rackley (eds), Feminist Perspectives on Tort Law (Routledge, 2012) 205; Martha Chamallas and Jennifer B Wriggins, The Measure of Injury: Race, Gender, and Tort Law (New York University Press, 2010)
ch 6.
[8] Brian C Murchison, ‘Treating Physicians as Expert Witnesses in Compensation Systems: The Public Health Connection’ (2002) 90 Kentucky Law Journal 891, 897–9 (on the importance of expert witness involvement and regulation for the integrity of compensation systems and their distributive justice function).
[9] Suzanne Burn and Sir Louis Blom-Cooper, ‘Remedies against the Defaulting Expert’ in Sir Louis Blom-Cooper (ed), Experts in the Civil Courts (Oxford University Press, 2006) 119, 119–20; Jennifer L Mnookin, ‘Expert Evidence, Partisanship, and Epistemic Competence’ (2008) 73 Brooklyn Law Review 1009, 1011.
[10] Jeffrey L Harrison, ‘Reconceptualizing the Expert Witness: Social Costs, Current Controls and Proposed Responses’ (2001) 18 Yale Journal on Regulation 253, 257–8, 262.
[11] See Mark Cooney, ‘Evidence as Partisanship’ (1994) 28 Law and Society Review 833, 851, suggesting that evidence is ‘the currency in which legal cases are transacted.’
[12] In sociological terms, brokerage is a process ‘by which intermediary actors facilitate transactions between other actors lacking access to or trust in one another’: Peter V Marsden, ‘Brokerage Behavior in Restricted Exchange Networks’ in Peter V Marsden and Nan Lin (eds), Social Structure and Network Analysis (Sage, 1982) 201, 202. See also Roger V Gould and Roberto M Fernandez, ‘Structures of Mediation: A Formal Approach to Brokerage in Transaction Networks’ (1989) 19 Sociological Methodology 89, 91.
[13] Victorian Law Reform Commission (‘VLRC’), Civil Justice Review: Report, Report No 14 (2008) 483; Lord Woolf, Department for Constitutional Affairs (UK), Access to Justice: Final Report to the Lord Chancellor on the Civil Justice System in England and Wales (1996)
137 [13.2].
[14] Gary Edmond, ‘Secrets of the “Hot Tub”: Expert Witnesses, Concurrent Evidence and Judge-Led Law Reform in Australia’ (2008) 27 Civil Justice Quarterly 51, 52–4.
[15] For a review of recent Australian reforms, see VLRC, above n 13, 488–98. See also Gary Edmond, ‘After Objectivity: Expert Evidence and Procedural Reform’ [2003] SydLawRw 8; (2003) 25 Sydney Law Review 131, questioning the simplistic images of objectivity motivating selected recent reforms and their empirical basis.
[16] Victoria, Parliamentary Debates, Legislative Assembly, 21 June 2012, 2947 (Robert Clark, Attorney-General). See also Civil Procedure Amendment Act 2012 (Vic) pt 3.
[17] Australian Law Reform Commission, Review of the Federal Civil Justice System, Discussion Paper No 62 (1999) 481 [13.2], 484 [13.16] <http://www.alrc.gov.au/dp-62> .
[18] One of the most notable exceptions is Australian Law Reform Commission, ALRC Part One: Empirical Information about the Administrative Appeals Tribunal, Research Report (1999) <http://www.alrc.gov.au/dp-62> , investigating the use of experts in Commonwealth and seafarers’ workers’ compensation and superannuation disputes.
[19] Gary Edmond and David Hamer, ‘Evidence Law’ in Peter Cane and Herbert M Kritzer (eds), Oxford Handbook of Empirical Legal Research (Oxford University Press, 2010) 652, 653.
[20] Nicola Y Cunningham and Tracey J Weiland, ‘Current Level of Training, Experience and Perceptions of Emergency Physicians as Expert Witnesses: A Pilot Study’ (2009) 21 Emergency Medicine Australasia 497; Tarryn Phillips, ‘“I Never Wanted to Be a Quack!” — The Professional Deviance of Plaintiff Experts in Contested Illness Lawsuits: The Case of Multiple Chemical Sensitivities’ (2010) 24 Medical Anthropology Quarterly 182; Bimal H Ashar, Redonda G Miller and Neil R Powe, ‘Extent and Determinants of Physician Participation in Expert Witness Testimony’ (2005) 98 Southern Medical Journal 444.
[21] Douglas Mossman and Marshall B Kapp, ‘“Courtroom Whores”? — Or Why Do Attorneys Call Us?: Findings from a Survey on Attorneys’ Use of Mental Health Experts’ (1998) 26 Journal of the American Academy of Psychiatry and Law 27.
[22] Anthony Champagne, Daniel Shuman and Elizabeth Whitaker, ‘An Empirical Examination of the Use of Expert Witnesses in American Courts’ (1991) 31 Jurimetrics Journal 375; Daniel W Shuman, Elizabeth Whitaker and Anthony Champagne, ‘An Empirical Examination of the Use of Expert Witnesses in the Courts — Part II: A Three City Study’ (1994) 34 Jurimetrics Journal 193; Carol Krafka et al, ‘Judge and Attorney Experiences, Practices, and Concerns regarding Expert Testimony in Federal Civil Trials’ (2002) 8 Psychology, Public Policy, and Law 309. Cf the investigation of judicial perceptions of expert evidence in Ian Freckelton, Prasuna Reddy and Hugh Selby, Australian Judicial Perspectives on Expert Evidence:
An Empirical Study (Australian Institute of Judicial Administration, 1999); Ian Freckelton, Prasuna Reddy and Hugh Selby, Australian Magistrates’ Perspectives on Expert Evidence:
A Comparative Study (Australian Institute of Judicial Administration, 2001).
[23] P Cornes and R C B Aitken, ‘Medical Reports on Persons Claiming Compensation for Personal Injury’ (1992) 85 Journal of the Royal Society of Medicine 329.
[24] Seth A Seabury, Robert T Reville and Frank Neuhauser, ‘Physician Shopping in Workers’ Compensation: Evidence from California’ (2006) 3 Journal of Empirical Legal Studies 47; Matthew Large and Olav Nielssen, ‘An Audit of Medico-Legal Reports Prepared for Claims of Psychiatric Injury Following Motor Vehicle Accidents’ (2001) 35 Australian and New Zealand Journal of Psychiatry 535.
[25] Samuel R Gross, ‘Expert Evidence’ [1991] Wisconsin Law Review 1113, 1119; Samuel R Gross and Kent D Syverud, ‘Don’t Try: Civil Jury Verdicts in a System Geared to Settlement’ (1996) 44 UCLA Law Review 1, 31–3; Amy P Walters, ‘Gender and the Role of Expert Witnesses in the Federal Courts’ (1994) 83 Georgetown Law Journal 635, 638, 643–4.
[26] Marilyn Price et al, ‘Gender Differences in the Practice Patterns of Forensic Psychiatry Experts’ (2004) 32 Journal of the American Academy of Psychiatry and the Law 250.
[27] Aaron S Kesselheim and David M Studdert, ‘Characteristics of Physicians Who Frequently Act as Expert Witnesses in Neurologic Birth Injury Litigation’ (2006) 108 Obstetrics and Gynecology 273.
[28] A treating expert’s evidence can be more akin to lay or eyewitness evidence than expert evidence, because it arises from a relationship located outside of the compensation context and because the parties are not able to control the identity of treating practitioners: Gross, above n 25, 1127 n 45; Murchison, above n 8, 907.
[29] For example, the disputation rate in workers’ compensation claims in Australia in 2009–10 was 4.7 per cent: Safe Work Australia, Comparative Performance Monitoring Report: Comparison of Work Health and Safety and Workers’ Compensation Schemes in Australia and New Zealand (13th ed, 2011) 37–8. The disputation rate indicates ‘the number of new disputes as a proportion of “active” claims in the reference financial year’, where a dispute is ‘an appeal to a formal mechanism, such as a review officer or conciliation or mediation service, against an insurer’s decision or decisions relating to compensation’ (but excluding common law claims and related disputes).
[30] See Gary Edmond, ‘Judging Surveys: Experts, Empirical Evidence and Law Reform’ [2005] FedLawRw 4; (2005) 33 Federal Law Review 95, 139 n 161, suggesting that ‘[m]ore attention ought to be devoted to the roles played by experts in the very large number of disputes that do not go to trial’.
[31] In the workers’ compensation context, Seabury, Reville and Neuhauser, above n 24, 54–5, note that ‘[c]ases with reports from multiple types of physicians are essentially disputed cases, and disputed cases are more likely to be cases that are “higher stakes,” or involve conditions with uncertain work causality or high subjectivity.’
[32] See, eg, Robert D Rondinelli (ed), Guides to the Evaluation of Permanent Impairment (American Medical Association, 6th ed, 2008) (‘AMA Guides’).
[33] See, eg, Katherine Lippel, ‘Compensation for Musculoskeletal Disorders in Quebec: Systemic Discrimination against Women Workers?’ (2003) 33 International Journal of Health Services 253, 277.
[34] Robert H Mnookin and Lewis Kornhauser, ‘Bargaining in the Shadow of the Law: The Case of Divorce’ (1979) 88 Yale Law Journal 950.
[35] See, eg, Champagne, Shuman and Whitaker, above n 22, 379 n 22, explaining that their study did not focus on experts involvement in settled cases because ‘the criticism of experts has been targeted at their use in the trial itself.’
[36] See Amos Tversky and Daniel Kahneman, ‘Availability: A Heuristic for Judging Frequency and Probability’ (1973) 5 Cognitive Psychology 207.
[37] But see Edmond’s critique of the dangers of privileging and reifying judicial perspectives on expert practice: Edmond, ‘Judging Surveys’, above n 30, 109–10.
[38] Content analysis is increasingly recognised as being suitable for use in legal research settings: see Mark A Hall and Ronald F Wright, ‘Systematic Content Analysis of Judicial Opinions’ (2008) 96 California Law Review 63.
[39] See, eg, Kesselheim and Studdert, above n 27; Gross, above n 25; Gross and Syverud, above
n 25; Walters, above n 25. Though some of these studies do not formally acknowledge that they used content analysis, the practices they describe are consistent with the method: see ibid 74, noting the regularity with which legal scholars undertake content analyses without reference to methodological literature.
[40] Hall and Wright, above n 38, 66.
[41] TAA s 12.
[42] TAA pt 3 div 3.
[43] TAA s 93(2). A serious injury is either a whole-person impairment of 30 per cent or more, or an injury that meets the narrative test set out in the Act: at ss 93(3), (17).
[44] Common law damages claims under the TAA are subject to a minimum threshold of $48 690 and maxima of $487 100 for non-pecuniary loss and $1 096 020 for pecuniary loss (as from
1 July 2012): ibid s 93(7); TAC, ‘Transport Accident Act Indexation of Benefits’ (Public Release, 2012) 1 <http://www.tac.vic.gov.au/upload/Indexation%20Public%20Copy.pdf> .
[45] For discussion of the development and operation of the pre-action protocols used in the TAC scheme, see VLRC, above n 13, 130–3.
[46] These applications may also include an application for extension of the time within which a claim may be brought: Limitation of Actions Act 1958 (Vic) s 23A.
[47] Damages claims may be brought in either the County Court or the Supreme Court of Victoria. Since the enactment of the Courts Legislation (Jurisdiction) Act 2006 (Vic) the County Court of Victoria has not been subject to a monetary limit on its jurisdiction: at s 3.
[48] Discussions with court staff indicated that the County Court of Victoria had published its transport accident serious injury decisions irregularly in recent years. It was possible, however, to identify a number of cases in which an unpublished judgment had been delivered, through review of the electronically searchable daily lists retained by the Court. These daily lists were available from early 2002 onwards. Accordingly, a study timeframe of 1 July 2002 – 30 June 2009 was established.
[49] Data provided by TAC by letter dated 9 April 2010 in response to the first author’s request pursuant to the Freedom of Information Act 1982 (Vic) dated 22 February 2010.
[50] The County Court uses circuit sittings to service communities in regional Victoria. In 2008, the Court reported that, at any one time, 20 per cent of its judges were engaged in circuit work, involving sittings in each of the 13 regional courts: County Court of Victoria, Annual Report 2007–08 (2008) 5 <http://www.countycourt.vic.gov.au/annual-reports> . The different listing and hearing procedures of the regional courts made it impossible to consistently or systematically identify non-Melbourne County Court decisions using the method described above. Additionally, the logistical difficulties associated with attending each of the 13 regional courts to obtain hard-copy decisions put non-Melbourne decisions beyond the scope of
the study.
[51] Since we completed our data collection, the County Court has started making its decisions available through the Australasian Legal Information Institute (‘AustLII’) website: AustLII, County Court of Victoria <http://www.austlii.edu.au/au/cases/vic/VCC> .
[52] In total, 110 unpublished decisions were obtained for the study.
[53] The relevant databases were the open access AustLII sites: AustLII, Supreme Court of Victoria <http://www.austlii.edu.au/au/cases/vic/VSC> AustLII, Supreme Court of Victoria — Court of Appeal <http://www.austlii.edu.au/au/cases/vic/VSCA> AustLII, Victorian Civil and Administrative Tribunal <http://www.austlii.edu.au/au/cases/vic/VCAT> . Additional searches of proprietary case databases (CaseBase and the Motor Vehicle Reports, both published by
LexisNexis) did not identify any further decisions. Additionally, to exclude the possibility that unpublished VCAT decisions existed, a selection of VCAT daily hearing lists was reviewed at the Tribunal. No further decisions were identified.
[54] These were all County Court decisions, and it is likely that many of these decisions were delivered ex tempore with no record retained for the court file.
[55] Non-expert decisions were principally about procedural matters, costs and other non-medical issues, such as the appropriate method for calculating the rate of a claimant’s
income benefits.
[56] Decisions excluded on this basis were most frequently Supreme Court of Victoria appellate reviews of VCAT decisions (n = 15) and Victorian Court of Appeal decisions relating to the County Court of Victoria’s serious injury decisions (n = 10).
[57] In a small number of instances where both an original decision and the decision on rehearing were available, only the more fulsome account of expert involvement in the proceeding was included in the study. Additionally, one claimant who was granted leave by the County Court to proceed with a common law damages claim then had that damages claim determined by a judge of the Supreme Court of Victoria. The evidence in these cases was very similar but was described in more detail in the judgment in the Supreme Court damages proceeding, so the County Court proceeding was excluded from the study.
[58] These matters were typically recovery proceedings, in which the TAC was the plaintiff seeking recovery of compensation paid to an injured person from the party whose negligence caused the relevant transport accident. The TAC is entitled to be indemnified by such a party ‘for such proportion of the amount of the liability of the Commission to make payments under this Act in respect of the injury or death as is appropriate to the degree to which the injury or death was attributable to [the negligent party’s] act, default or negligence’: TAA s 104(1). Recovery proceedings have a fundamentally different focus than the other claims in the study dataset, with the TAC acting as plaintiff rather than defendant, so these decisions were
excluded.
[59] In decisions with concurrent workers’ compensation claims it was not possible to determine which experts had been engaged for the purposes of the transport accident claim. To include these decisions would have violated the sampling frame’s focus on transport accident compensation cases.
[60] VLRC, above n 13, 130, 132; TAC, Together, We Achieve: Annual Report 2006 (2006) 20–1 <http://www.tac.vic.gov.au/about-us/annual-reports> .
[61] This definition encompassed health practitioners who, as at 1 July 2011, were eligible to register under the relevant health practitioner law in the state or territory in which they resided: Health Practitioner Regulation National Law (ACT) Act 2010 (ACT); Health Practitioner Regulation (Adoption of National Law) Act 2009 (NSW); Health Practitioner Regulation (National Uniform Legislation) Act 2010 (NT); Health Practitioner Regulation National Law Act 2009 (Qld); Health Practitioner Regulation National Law (South Australia) Act 2010 (SA); Health Practitioner Regulation National Law (Tasmania) Act 2010 (Tas); Health Practitioner Regulation National Law (Victoria) Act 2009 (Vic); Health Practitioner Regulation National Law (WA) Act 2010 (WA).
[62] Experts were excluded where they were noted on a list of practitioners scheduled to the decision but not referred to in the decision itself.
[63] Some decisions made reference to reports produced for a claimant’s prior workers’ compensation or victims of crime compensation claim. These reports and experts were excluded. Additionally, where a practitioner had merely corresponded with the claimant’s treating practitioner rather than actually producing a report for the purposes of the litigation, they were excluded.
[64] The definition also includes midwives, nurses and pharmacists, but there were no expert witnesses from these practitioner categories in the dataset. Several categories of practitioners provided reports in study cases but were excluded because of their non-registrable status. Occupational therapists (n = 12) were excluded as they were non-registrable as at 1 July 2011 (the registration requirement for occupational therapists commenced on 1 July 2012). Other non-registrable practitioners who provided reports in the study dataset cases were vocational consultants and assessors (n = 5), audiologists (n = 2), masseurs (n = 2) and social workers
(n = 2).
[65] AHPRA, Registers of Practitioners <http://www.ahpra.gov.au/Registration/Registers-of-Practi tioners.aspx> .
[66] For example, the Royal Australasian College of Surgeons In Memoriam site, which lists Fellows of the College who have died since 2006, was particularly useful for this purpose: Royal Australasian College of Surgeons, In Memoriam <http://www.surgeons.org/member-services/in-memoriam> . The main reasons experts were not registered seemed to be because they had relocated overseas, been subject to disciplinary action, retired or died.
[67] Despite the fundamental differences between treating and non-treating experts identified above, treating practitioners are regarded as experts where they provide their expert opinion on their patient: Ian Freckelton and Hugh Selby, Expert Evidence: Law, Practice, Procedure and Advocacy (Lawbook, 4th ed, 2009) 239, noting that treating experts ‘possess specialised knowledge based upon their training, study or experience’, consistent with legal definitions
of expertise.
[68] This is particularly the case with respect to expert evidence obtained by the defendant TAC, which, as an entity subject to the Freedom of Information Act 1982 (Vic), is effectively in the position of having to disclose all medical reports it obtains in relation to a claimant. However, claimants are able to determine whether unfavourable expert evidence they have obtained will be withheld from the TAC, in reliance on lawyer–client privilege: see Evidence Act 2008 (Vic) s 118.
[69] Administrative details included the case name, adjudicator’s name, decision date and the plaintiff or applicant solicitor firm name (or self-represented status).
[70] A kappa score is a rating of ‘the proportion of agreement after chance agreement is removed from consideration’: Jacob Cohen, ‘A Coefficient of Agreement for Nominal Scales’ (1960) 20 Educational and Psychological Measurement 37, 40 (emphasis in original). Landis and Koch propose that scores between 0.61 and 0.80 demonstrate ‘substantial’ agreement, with scores of 0.81 to 1.00 being ‘almost perfect’: J Richard Landis and Gary G Koch, ‘The Measurement of Observer Agreement for Categorical Data’ (1977) 33 Biometrics 159, 164–5.
[71] Data provided by the TAC indicate that in the study period, 34 damages claims were resolved by the County Court of Victoria and nine by the Supreme Court of Victoria in the entire State of Victoria (data provided to the author by TAC by letter dated 9 April 2010 in response to a request pursuant to the Freedom of Information Act 1982 (Vic) dated 22 February 2010). There was, however, only one damages decision in the study dataset (a Supreme Court decision). The disparity between the statewide number of damages decisions reported by the TAC and the study dataset can be explained by the study’s focus on claims in Melbourne; the availability of civil jury trials in Victoria (for which there would be no decision record detailing expert involvement); and the possibility that damages judgments may have been delivered ex tempore, without a written record being retained by the court.
[72] Mathematically, the total number of expert involvements in the study sample is equivalent to the number of cases multiplied by the number of unique experts engaged in those cases. By ‘unique’ experts, we mean that no expert could be counted as having more than one involvement in any single case. This is somewhat artificial in the sense that experts may have provided more than one report over the life of a claim. This counting convention was adopted partly for conceptual reasons (we were interested primarily in the engagement of experts by case, rather than their precise role within cases) and partly for feasibility reasons (our data did not permit reliable identification of specific expert activities within cases).
[73] The ‘other non-surgeon’ category in Figure 2 includes psychologists, gastroenterologists and hepatologists, respiratory and sleep medicine physicians, cardiologists, urologists, ophthalmologists, physiotherapists, addiction medicine specialists and chiropractors.
[74] Surgical expert witnesses appearing in the sample included orthopaedic surgeons, vascular surgeons, general surgeons, neurosurgeons, plastic surgeons, otolaryngologists (head and neck surgeons) and cardiothoracic surgeons. The AHPRA register failed to report a surgical specialty for 6 per cent of surgeons (n = 53, all male).
[75] Cf Kesselheim and Studdert, above n 27, 274–5, classifying witnesses who provided evidence in more than 10 cases in a sample of 738 neurological birth injury cases over a 15-year period in the United States as ‘frequent witnesses’.
[76] The AHPRA register does not record practitioner age or date of birth, but it does record date of first registration. Our approach to approximating expert age was based on an assumed age at first medical profession registration of 24 years (consistent with entry into an undergraduate medical degree course at age 18 for a six-year course of study). For frequent experts not listed on the AHPRA register, searches of the National Library of Australia Trove Repository: National Library of Australia, Trove <http://trove.nla.gov.au> , newspapers and the web were additional sources for determining the expert’s year of birth. For example, several frequent experts had produced postgraduate theses and these were evident in Trove records along with the year of the expert’s birth. This data confirmed the accuracy of the age approximation technique adopted for the study. Consistent with the approach adopted by Kesselheim and Studdert, the case-specific age of each expert was calculated at the date on which each of their respective cases was determined: Kesselheim and Studdert, above n 27, 275. The average age of the expert during the study period was then determined by averaging the case-specific
age values.
[77] We determined each FE’s annual case rate by dividing their total number of cases by the number of years that elapsed between the FE’s first and last study cases.
[78] It was not possible to obtain specialty and age data on five of the 69 FEs. Therefore all age and specialty calculations are based on the 64 FEs on whom we had this information. Gender, on the other hand, was available for all 69 FEs.
[79] Australian Institute of Health and Welfare (‘AIHW’), Additional Material: Medical Labour Force Time Series 1997 to 2009 table A15 ‘All Specialists (Clinician and Non-Clinician): Selected Characteristics by Main Specialty of Practice, Australia, 1997 to 2009’ in AIHW, Medical Labour Force 2009 (Catalogue No AUS 138, 19 August 2011) <http://www.aihw.gov.au/ publication-detail/?id=10737419680 & tab=3> , showing that, Australia-wide, 21.9 per cent of medical specialists were female in 2006. We have used the Medical Labour Force data in this and subsequent comparisons. We chose to use this national-level dataset rather than a Victorian dataset because the national data includes clinicians and non-clinicians. The results would not be markedly different had we used the Victorian data, however: see Department of Human Services (Victoria), ‘The Victorian Medical Workforce 2000–2006’ (Report, May 2009) chs 4–5. We chose 2006 data to account for the variable years of cases in the
study sample.
[81] Ibid. Within the surgical specialty, the national mean ages for the major subspecialties represented in the study sample were as follows: orthopaedic surgeons, 51 years; neurosurgeons, 51 years; general surgeons, 54 years; vascular surgeons, 52 years; and plastic surgeons, 51 years.
[82] This table omits the 63 involvements in which the gender of the non-treating expert
was unknown.
[83] In two instances, the gender of a non-treating expert who gave viva voce evidence
was unknown.
[84] See, eg, Australian Bureau of Statistics, ‘Selected Health Occupations: Australia, 2006’ (ABS Catalogue No 4819.0, 17 June 2008).
[86] See Figure 1, above Part IIIB.
[87] Australian Law Reform Commission, above n 18, 32. Study cases were finalised during August, September and October 1997: at 5 [1.2]. ‘Compensation’ cases were those involving Commonwealth and seafarers’ workers’ compensation and superannuation disputes: at 45. Data on expert involvement was based on ‘the number of experts who provided an expert report or who were to be called to give oral evidence at a hearing, as evidenced by the information on hearing certificates’: at 31. Though their study was not focused solely on medical experts, the authors noted the importance of medical experts to the compensation cases:
at 31. There was a median of two experts used by each side in the compensation cases: at 32.
[88] Consider the different subjects of measurement in the following examples: in the personal injury trials featuring in a study of Californian jury verdicts, there were on average 3.8 experts per case, only around 60 per cent of whom were health practitioners: Gross, above n 25, 1119. In a later sample comprising injury and non-injury claims, the mean number of all experts (medical and non-medical) testifying per case increased from 3.3 in 1985–86 to 4.1 in
1990–91: Gross and Syverud, above n 25, 31–2. In a study of federal civil trials in the United States in 1998, an average of 4.3 experts testified per trial (45 per cent of study cases were tort cases, and 40 per cent of experts were mental health and medical specialists): Krafka et al, above n 22, 319–20. In the United Kingdom, a study of small claims found that expert reports, most of which were medical, were commissioned in over 90 per cent of cases, but there were on average only 1.6 reports per case and in only 1 per cent of cases were more than 5 reports commissioned. Less than 1 per cent of the sample actually went to trial, however: Pascoe Pleasence, Report of the Case Profiling Study: Personal Injury Litigation in Practice (Legal Aid Board Research Unit, 1998) 47, 52–3.
[89] Pleasence, above n 88, 18.
[90] Katherine Lippel, ‘Workers Describe the Effect of the Workers’ Compensation Process on Their Health: A Québec Study’ (2007) 30 International Journal of Law and Psychiatry 427, 437; Ellen MacEachen et al, ‘The “Toxic Dose” of System Problems: Why Some Injured
Workers Don’t Return to Work as Expected’ (2010) 20 Journal of Occupational Rehabilitation
349, 356.
[91] The majority of the study cases were serious injury decisions of the County Court of Victoria. Three quarters of those cases were determined six or more years after the claimant’s accident date, and more than a third were determined eight or more years post-accident (authors’ calculations based on the time elapsed between the transport accident and case decision data in each of the County Court decisions in the sample).
[92] See, eg, VLRC, above n 13, 511; Dodoro v Knighting [2004] VSCA 217; (2004) 10 VR 277, 291 [56] (Eames JA).
[93] For example, one interesting trend in civil litigation is to have witnesses present their testimony concurrently. Proponents of this approach posit that the method, referred to colloquially as ‘hot tubbing’, improves the veracity and quality of expert evidence: see generally Edmond, ‘Secrets of the “Hot Tub”’, above n 14.
[95] See CSR Ltd v Della Maddalena [2006] HCA 1; (2006) 224 ALR 1, 13 [39] (Kirby J) (on the reality of experts becoming ‘well known to the court’); Vakauta v Kelly [1989] HCA 44; (1989) 167 CLR 568, 570 (Brennan, Deane and Gaudron JJ), 576 (Dawson J). There would be less familiarity for claimants in cases involving litigants in person (in this study, n = 14) and less experienced plaintiff solicitors, who would be less likely to have access to knowledge about experienced and appro-priate experts.
[96] Gary Edmond, ‘Judicial Representations of Scientific Evidence’ (2000) 63 Modern Law Review 216, 235.
[97] VLRC, above n 13, 90, 92–4.
[99] Mnookin, above n 9, 1014–15.
[100] Law reform commission reports, for instance, have focused on the perceived impact of ‘adversarial bias’: see, eg, New South Wales Law Reform Commission, Expert Witnesses, Report No 109 (2005) 71–4 [5.5]–[5.15]; VLRC, above n 13, 484, noting that adversarial bias is ‘an inevitable feature of a system in which courts must arrive at decisions about complex questions of fact based on the competing views of opposing experts.’
[101] Edmond, ‘Judging Surveys’, above n 30, 136.
[102] See, eg, Robert H Brook, Elizabeth A McGlynn and Paul D Cleary, ‘Measuring Quality of Care’ (1996) 335 New England Journal of Medicine 966; Robert H Brook, Elizabeth A McGlynn and Paul G Shekelle, ‘Defining and Measuring Quality of Care: A Perspective from US Researchers’ (2000) 12 International Journal for Quality in Health Care 281.
[103] See, eg, Jane Goodman-Delahunty and Mandeep K Dhami, ‘A Forensic Examination of Court Reports’ (2013) 48 Australian Psychologist 32, 35–8, describing the decisions made by experts writing forensic psychology reports, and their impact on report content.
[104] See, eg, Ralph B Blasier, ‘The Problem of the Aging Surgeon: When Surgeon Age Becomes a Surgical Risk Factor’ (2009) 467 Clinical Orthopaedics and Related Research 402, 404–5, describing the contribution of age-related cognitive and physical decline to the degradation of surgical skills.
[105] See Mnookin, above n 9, 1011, suggesting that ‘those witnesses who succeed in the marketplace for experts within our adversarial process will often not be those with the most knowledge or actual expertise in a particular area, but rather those whom parties believe will succeed in persuading the factfinder.’
[106] Francesca Bartlett, ‘Model Advocates or a Model for Change? The Model Equal Opportunity Briefing Policy as Affirmative Action’ [2008] MelbULawRw 12; (2008) 32 Melbourne University Law Review 351, 351–2.
[107] Regina Graycar and Jenny Morgan, The Hidden Gender of Law (Federation Press, 2nd ed, 2002) 422–4.
[108] Debra L Roter, Judith A Hall and Yutaka Aoki, ‘Physician Gender Effects in Medical Communication: A Meta-Analytic Review’ (2002) 288 Journal of the American Medical Association 756.
[109] Ibid 761.
[110] Ibid 763.
[111] In particular, Roter, Hall and Aoki focused on studies in the primary care context: ibid. Expert witnesses are predominantly medical specialists, and there has been little empirical study of gender differences in the communication practices of medical specialists.
[112] TAA s 93(17).
[113] See, eg, Jacqueline Scott, Anke C Plagnol and Jane Nolan, ‘Perceptions of Quality of Life: Gender Differences across the Life Course’ in Jacqueline Scott, Rosemary Crompton and Clare Lyonette (eds), Gender Inequalities in the 21st Century: New Barriers and Continuing Constraints (Edward Elgar, 2010) 193.
[114] Price et al, above n 26, 251.
[115] See Andrew E Taslitz, ‘What Feminism Has to Offer Evidence Law’ (1998) 28 Southwestern University Law Review 171, 179–80.
[116] See ibid 188, noting that in the competitive market metaphor of the trial, ‘externalities — costs imposed on society but not on the parties to the litigation — are either assumed not to exist or to be irrelevant.’
[117] Edmond suggests that ‘[u]navoidably, judgments are summaries. Emphases, however, like inclusions and omissions, are not arbitrary’: Gary Edmond, ‘Judging Facts: Managing Expert Knowledges in Legal Decision-Making’ in Gary Edmond (ed), Expertise in Regulation and Law (Ashgate, 2004) 136, 147.
[118] See the discussion above at Part II.
AustLII:
Copyright Policy
|
Disclaimers
|
Privacy Policy
|
Feedback
URL: http://www.austlii.edu.au/au/journals/MelbULawRw/2013/2.html